Introduction
Tactical Rabbit is a Private Intelligence Agency I founded after the HSBC terrorist and drug cartel scandal in 2012. I witnessed billions of dollars going to terrorists and cartels. The terrorist money was being used to make the IED’s to blow up American troops. I passed information to the CIA and FBI for over a year and my evidence led to the largest fine in U.S. History against a bank. Unfortunately, nobody went to jail. In response, I formed Tactical Rabbit to promote Justice, Fight Corruption, and Hold People Accountable.
I formed a Tactical Rabbit National Security Division that collects intelligence and fills in intelligence gaps of the United States Government. The work of the National Security Division also launches and produces intelligence reports for the American public as I am a firm believer in exposure and making sure the American People are aware of what is really happening.
The National Security Division is fully self-financed by people contributing to the cause of promoting justice and exposing what is wrong to bring about corrective action. Please join the fight by contributing to the Tactical Rabbit National Security Division and by subscribing to this Substack. Wars cost money and we need financing to fight the good fight.
Thank you for fighting alongside of us. It is an honor to serve with you on the battlefield. -Everett A. Stern
INTELLIGENCE REPORT: Michigan
Executive Summary:
Using documents obtained through the Freedom of Information Act (FOIA) and other many other reputable sources, we have undoubtedly identified three acts of intentional fraud carried out by the Michigan Department of Health and Human Services (MDHHS) that took place during the term of outgoing Governor, Rick Snyder. The schemes resulted in millions of taxpayer dollars being monopolized and likely, the denial of care for countless members of Michigan’s elderly population. The impact of this is immense amounts of untold suffering and has likely led to many individuals being prematurely placed in institutional care at great human, medical and fiscal cost. Our findings are the tip of the iceberg of the out-of-control state bureaucracy driven by civil servants and political appointees more interested in protecting their personal freedoms than in delivering top-quality health care to the state’s most vulnerable residents. This is a human crisis unrecognized by most officials.
II. Background:
Our findings surround the Flint Water crisis that has left at least 28 people dead of Legionnaires’ Disease, numerous seriously injured and countless children suffering from the long-term consequences of lead poisoning.
MDHHS Director Nick Lyon has been indicted on two counts of involuntary manslaughter and official misconduct for his mishandling and the intentional cover-up of the Flint situation. In August 2018, a District Court Judge found that Lyon was “corrupt” in his handling of the Flint-area Legionnaires’ disease outbreak. The judge ruled that Lyon “willfully and neglectfully refused” to protect the lives of two Flint area men who died from Legionnaires’ disease, by failing to notify the public of the outbreak after the Flint drinking water crisis went public. Shockingly, he remains in office, free on bail, with taxpayers paying the well-over $1.6 million for his legal defense bills. It was on Lyon’s watch that these three acts of fraud occurred, crimes that have so far been ignored, with the named and unnamed perpetrators still on the payroll, collecting paychecks and continuing to inflict harm.
Like the victims of Flint, the victims of these frauds are a very vulnerable group – elderly, frail and disabled people who require help with daily living skills.
www.TacticalRabbit.com Michigan Page 3 of 10
CONFIDENTIAL TACTICAL RABBIT, INC
III. Key Judgments:
– In 2010, MDHHS officials were rolling out a new computer program “Edit 1221” as part of ongoing implementation of CHAMPS (Community Health Administrative Management System), the system was designed to streamline billing, payment, and held the responsibility of tens of millions of dollars a year in annual home health services for people requiring assistance with daily living skills including bathing, eating, dressing, toileting, mobility, and other Medicaid approved non-medical services.
In home care is a growing phenomenon across the country designed to allow patients, especially seniors, to avoid institutionalized care and retain independence for as long as possible. The program has demonstrated medical and humanitarian benefits and results in massive financial savings. A review of typical billings for at home care indicates that Medicaid frequently paid for only two hours of service per day – an average of $1,120 per month, as compared to $7,900 per month in fees that accrue from an individual residing in a nursing home.
– In June of 2010, the program “Edit 1221” was producing numerous errors. A decision was made to disable the software, rather than resolve the error in the system. According to email from MDHHS, secured under the Freedom of Information Act (FOIA), a bureaucrat made this decision “to ease the burden on claims processing staff”, with no reference to patient care or fiscal implications. This allowed home health aid payments to be made without further review, payments were automatically generated and delivered without verification that appropriate care was being provided.
– Millions of dollars in potentially unscreened, illegitimate payments, were processed. Had it not been disabled, “Edit 1221” would have impeded these transactions. Due to the lack of an evaluation process, it is essentially impossible to tell if patients were receiving appropriate services. It can be assessed that the improper figures representing in home services and nursing/therapy costs led families to send loved ones to nursing homes prematurely and prevented many from receiving any appropriate care. It is unknown at what level the decision was cleared, or if Washington was consulted to determine if the action took MDHHS out of federal compliance.
– In 2017, MDHHS discovered that the program had been disabled, seven years earlier. Instead of reporting the years of erroneous activity to proper authorities, a small group of MDHHS bureaucrats launched a cover-up operation that included a straw horse attack on a well-respected provider to divert attention from their mismanagement. The cabal unleashed an audit of the provider by the Office of Inspector General (“OIG”), rather than asking for an outside review of their own internal errors. Their actions make it clear that there was no intention to either fully brief state or federal OIGs or to contact any other law enforcement agency about the possible criminal implications of the situation.
-We assess that the aforementioned policy specialist has a record of overstepping her bounds. In 1993, she appealed a demotion for a job then described as “Departmental Specialist VIII,” a job description similar to the current post. The demotion was made after a supervisor determined that the specialist “cannot be, and is not…perceived or recognized as an expert; but more approximately should be recognized as a Resource Person/Troubleshooter.
– The OIG later asked the policy office for clarification as to whether there had been any update to rules governing restrictions on home health aide payments. Emails indicate the state continued to insist there had been no such update. This was a misstatement. In February 2016, federal officials changed Medicaid regulations to allow more people to obtain home health services. It could not be determined if the information sent to the OIG was a deliberate misstatement or an error.
– More than two years after federal officials mandated changes to state programs intended to deliver more home services to patients, the MDHHS providers’ manual continues to use the outdated requirements. It is unclear how many elderly Michigan patients are not receiving services to which they are entitled. It is also unclear how many Michigan patients have been forced into institutional settings because of the failure to update the manual. And it is also unclear how many millions of dollars have been wasted.
IV. Additional Background Data:
When Medicaid was launched in 1965, it was designed to provide medical services for the elderly and disabled, the most vulnerable residents in our nation. The nature of care and service models have evolved over the years. In the 1960s, the model focused on institutional care. Over the past decade, medical professionals and advocates recognized the benefits of keeping people in their own homes and out of institutions. Remaining at home brings seniors a better quality of life. And it saves taxpayers money.
Originally, home help services were only provided to patients receiving skilled nursing and physical therapy. That model was failing patients suffering short-term difficulties like broken bones or sprains or even short-term illnesses from which they were expected to recover. During the recovery period, Medicaid pays for aides to assist patients who have trouble with daily living skills – dressing, getting in and out of bed, toileting, bathing etc.
The original computer model – Edit 1221 – was designed to make sure that every home health bill had attached documentation of ongoing nursing and/or therapy service.
Over the years, advocates claimed that many elderly people had different needs. Many aging patients require assistance with daily living skills, because of aging-driven problems that cannot be addressed with therapy. The required link [to skilled nursing and physical therapy] made no sense, advocates said.
While the debate about adopting a new model was underway in Washington, Lansing decided it was easier to stick with the old model – ignoring the possible medical and financial benefits of unlinked home and health services. It is not clear just how many Michigan residents were forced into nursing homes because of this outdated thinking.
On Feb. 2, 2016, Washington issued new guidelines; no longer were Home Health aide services linked to nursing and therapy. They would from that day forward be made available to a larger population of folks facing the vagaries of old age.
MDHHS ignored the directive for at least two years. After the March 2017 discovery that Edit 1221 had been disabled, policy staff insisted in emails to superiors that no such update had been issued by Washington.
In March 2018, the OIG again asked the policy office if aide payments required linkage to nursing/therapy. A policy analyst said it did, even though that same person was preparing a bulletin announcing the belated Washington-ordered change. At the time the analyst was facing serious charges by the state board of nurses relating to alleged failure to report serious injury to a nursing home patient. Although those charges were later dismissed, they were very much alive at a time the cover-up was being hatched.
On May 25, 2018, the state’s policy office issued a “Clarification” bulletin to home health aide providers stating, “home health aide services cannot be contingent upon the beneficiary needing nursing or therapy services.” Despite the announcement and a subsequent similar bulletin issued in August 2018, the current version of Michigan’s provider handbook, published in October 2018, still insists on compliance with the now- outdated regulation. It states: “home health aide services are covered only when ordered by the attending physician and performed in conjunction with direct, ongoing skilled nursing care and/or PT.”
The order for home help services comes from the patient’s doctor (or physician’s assistant) and is given to registered Medicaid providers who employ the aides. The provider bills the state monthly on a fixed per-hour fee for services provided.
Originally, home help services were only provided to patients receiving skilled nursing and physical therapy. That model was good for patients suffering short-term difficulties like broken bones or sprains or even short-term illnesses from which they were expected to recover. During the recovery period, Medicaid pays for aides to assist patients who have trouble with daily living skills – dressing, getting in and out of bed, toileting, bathing etc.
The original computer model – Edit 1221 – was designed to make sure that every home health bill had attached documentation of ongoing nursing and/or therapy service.
Over the years, advocates claimed that many elderly people had different needs. Many aging patients require assistance with daily living skills, because of aging-driven problems that cannot be addressed with therapy. The required link [to skilled nursing and physical therapy] made no sense, advocates said.
While the debate about adopting a new model was underway in Washington, Lansing decided it was easier to stick with the old model – ignoring the possible medical and financial benefits of unlinked home and health services. It is not clear just how many Michigan residents were forced into nursing homes because of this outdated thinking.
On Feb. 2, 2016, Washington issued new guidelines: No longer were Home Health aide services linked to nursing and therapy. They would from that day forward be made available to a larger population of folks facing the vagaries of old age.
MDHHS ignored the directive for at least two years. After the March 2017 discovery that Edit 1221 had been disabled, policy staff insisted in emails to superiors that no such update had been issued by Washington.
In March 2018, the OIG again asked the policy office if aide payments required linkage to nursing/therapy. A policy analyst said it did, even though that same person was preparing a bulletin announcing the belated Washington-ordered change. At the time the analyst was facing serious charges by the state board of nurses relating to alleged failure to report serious injury to a nursing home patient. Although those charges were later dismissed, they were very much alive at a time the cover-up was being hatched.
On May 25, 2018, the state’s policy office issued a “Clarification” bulletin to home health aide providers saying:
“Home health aide services cannot be contingent upon the beneficiary needing nursing or therapy services.”
Despite that “clarification” and a subsequent similar bulletin issued in August 2018, the current version of Michigan’s provider handbook, published in October 2018, still insists on compliance with the now outdated regulation. It states: “Home health aide services are covered only when ordered by the attending physician and performed in conjunction with direct, ongoing skilled nursing care and/or PT.”
V. Intelligence Analysis:
Our findings suggest that the administration within Michigan Department of Health and Human Services knowingly, willingly, and intentionally participated in defrauding taxpayers and failed to comply with federal legislation. The schemes resulted in countless members of Michigan’s elderly population being unable to receive care they desperately needed and an indeterminate financial contribution from innumerous taxpayers for illicit causes, beyond their knowledge. The impact of this has undoubtedly led to immense amounts of untold suffering and has likely led to many individuals being prematurely placed in institutional care at great human, medical and fiscal cost. Our findings are just a hint of what occurs within this out-of-control state bureaucracy driven by self-interested political appointees who have no dilemma in foregoing the needs of our societi’s most vulnerable individuals for their own gain. This is a human crisis, in every sense. Due to the failure to investigate the program being halted, potentially against federal legislation, the complete impact of this is unknown but is anticipated to be detrimental; financially, physically, and emotionally to those impacted by these blatant failures to take responsibility for actions taken with selfish intentions. Further investigation into improper filings, leadership, employees, and more, is urgently necessary to expose the years of damage and corruption within these processing procedures.
“Flint Pipes released as much as 18 grams of Lead, per household.”
Image depicting Flint water pipes.

“Former Michigan Gov. Rick Snyder pleaded not guilty to misdemeanor charges he willfully neglected his duty during the Flint water crisis. Eight other former officials and aides were also charged in connection to the scandal.”
Flint water crisis turns skin condition into daily pain for resident of the city.
“A little shortcut to save them money, while you’re destroying people’s lives… I can’t regain my trust. I really can’t. I feel like this situation with me trying to get help, they don’t really care,
they just don’t care.”
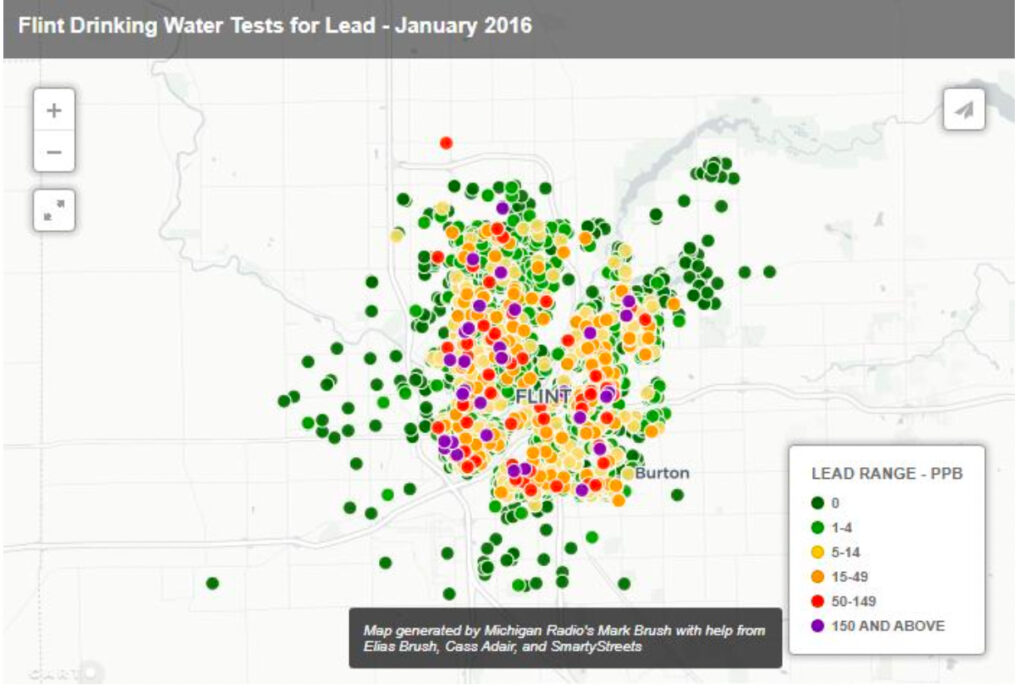
“The addresses of 4,051 drinking water tests in Flint for the month of January. The lead results
were grouped into six ranges.”
0 ppb: no lead detected in the drinking water
1-4 ppb: the EPA deems this range as acceptable
5-14 ppb: exposure is a concern, but still below an EPA “federal action level”
15-49 ppb: a range above the federal action level for lead, but can be treated by filters 50-149 ppb: reaching dangerous levels, but can be treated by filters
150 and above: a range at which the federal government says water filters might not work
www.TacticalRabbit.com Michigan Page 10 of 10